Ankle sprains are one of the most common injuries among physically active people accounting for an estimated 23,000 sprains -- daily --that are attributed to athletic activity. (1) Basketball players suffer the highest incidence rate among sports (41.1%) followed by football (9.3%), soccer (7.9%), running (7.2%) and volleyball (4.0%). Unlike the knee and ACL injuries there is no predilection to females over males with ankle sprains occurring 50.3% and 49.7% respectively. (2) Nearly 30% of first time ankle sprains will cause chronic ankle instability (CAI) which has also been reported as a contributing factor to the early onset of osteoarthritis. (3) The effects of CAI are also seen beyond the local area of injury as altered pelvic stability. Although ankle sprains are typically treated in the physical therapy setting there are many things a personal trainer can do to help restore full function and also prevent future injuries.
A history of a previous ankle sprain is the most common predictor of this type of injury, with an incidence rate of 73%. This injury most often occurs when landing either on the ground or on another player’s foot. (4) Other causes include a sharp turn or twist, collision, fall or sudden stop. This results in functional deficits including range of motion, limited ankle dorsiflexion, impaired proprioception and balance control, and increased pelvic neuromuscular reaction time. (5,6)
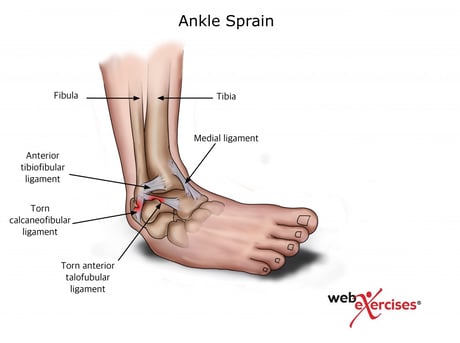
In order to understand what exercises would be best, a brief review of the anatomy is necessary to understand the structures involved with this type of injury. Since 70% to 85% of ankle sprains occur to the lateral side of the ankle this article will focus on exercises based around this location. (7) The most commonly injured ligaments consist of the anterior talofibular, calcaneofibular and posterior talofibular ligaments which connect the talus and calcaneus with the fibula. (17) The tendon of the peroneal muscle, which is responsible for foot eversion, is also commonly strained with inversion injuries as it runs superficial to the posterior talofibular and calcaneofibular ligaments.
Before starting an exercise program it is important to determine what type of functional ankle instability issue your client may have. This can include ligamentous laxity, decreased dorsiflexion, or proprioceptive, balance or strength deficits.
In order to determine if there is ligament laxity, passive range of motion is a simple way to assess this. To perform, begin with the client in a non-weight bearing position in order to eliminate any muscular influence, then move the ankle through all ranges of motion including plantar flexion, dorsiflexion, inversion, eversion, internal rotation and external rotation. Perform bilaterally noting any differences from one side to the other.


Dorsiflexion Assessment
Next assess dorsiflexion as this has been reported as a potential risk of re-injury. It affects how your client walks, jogs or performs other functional and daily activities. (8) The normal range for dorsiflexion is 20 to 24 degrees. A simple way to assess if your client is within this range is to have them get into a half kneeling position with a dowel perpendicular to the floor, four inches in front of their great toe. Have them glide forward while keeping their heel firmly on the floor and measure how close their knee comes to the dowel. Repeat on the opposite side to compare the results.
Once a baseline has been established this assessment can also be used as a method to help improve posterior talar glide and dorsiflexion. Vencenzo and colleagues demonstrated an increase in dorsiflexion range of motion after a series of mobilization exercises, one of which is similar to the above. (18) Perform 3 sets of 12 repetitions 2-3 times per day.
It is well established in the literature that proprioception is affected after ankle sprains, impairing joint position sense, predisposing one to re-injury. (10) This can be caused by either an unanticipated foot position when stepping on an uneven surface or as a result of improper foot positioning in space prior to ground contact. An easy way to assess this is to perform a single leg balance test with eyes open and then again with eyes closed, comparing bilaterally. The chart below provides the normative values for each age group.


Single Leg Balance Assessment - Bend one leg at the knee, lifting the foot off of the ground. If necessary, grasp chair for additional stability. Attempt to balance for 30 seconds. Note the time and any differences between sides.
| Age
|
Eyes Open
|
Eyes Closed
|
| 20-59 | 25-30 sec. | 21-28 sec. |
| 60-69 | 22 sec. | 10 sec. |
| 70-79 | 14 sec. | 4 sec. |
Single Leg Balance Test Normative Values (11-15)
As with the previous assessment, this can also be used as an exercise to improve your client’s balance. After they are able to balance at the time values indicated above, they can be progressed to a balance board, which has been shown to be effective in ankle rehabilitation. Verhagen and colleagues demonstrated that balance board training was effective in preventing a recurrence of ankle sprains with Dutch volleyball teams who performed a series of exercises over the course of the season. Balance board exercises can also be progressed by adding a medicine ball toss.
However, specificity should also be considered before the athlete returns to their sport as some authors suggest balance assessment and activities that are task specific to their activity should be performed. (16) An example of this would be to have a gymnast assess on the balance beam or other activities specific to their sport.


Balance Board Training - Begin standing with two feet on a balance board. Activate core as you raise your opposite foot so you are balancing on one foot not letting the edges of the board touch the ground. Hold for up to 30 seconds and repeat 3 times.
Although the literature is unclear to what degree strength is affected by chronic ankle instability it would be prudent to include a simple peroneal strengthening exercise given these tendons are commonly strained with inversion injuries. (21)


Ankle Eversion with Resistance Band - Begin seated in a chair with a resistance band around forefoot (opposite end of resistance band anchored to a firm, non-moving, structure). Knees should also be at 90 degrees. While maintaining the alignment of the kneecap and second toe, lift forefoot off the floor and move outward in a scooping type motion against resistance band. Slowly return to start position and repeat without resting foot on floor. Perform 3 sets of 12 repetitions.
Pelvic stability is also influenced by chronic ankle sprains as Friel and colleagues demonstrated in their study. Evaluating individuals with a history of at least two (2) ankle sprains, but not experiencing symptoms at the time, they found the strength of the hip adductors were significantly weaker on the side on the ankle sprain.
Another study, by Beckman and Buchanan, showed increased neuromuscular reaction time of the hip abductors. Their research demonstrated latency differences in the gluteus medius on the side of ankle hypermobility in subjects. (20) These concomitant factors in turn change the position of the pelvis during gait and subsequently require the body to develop compensation strategies. This leads to alteration in the lower body kinetic chain that at some point will break down.
To help prevent or avoid this break down hip adductor and abductor exercises are recommended. The side lying hip adduction is a good starting point to isolate the adductor muscle group.


Side Lying Hip Adduction - Begin lying on side with hand supporting head. Bottom leg is straight, top leg knee is bent and placed behind straight leg with foot flat on the floor. Activate core muscles. Lift straight leg upward six to eight inches and slowly return to start position. You should feel the muscles of the inner thigh working. Perform 3 sets of 12 repetitions.
Activating the gluteus medius can be performed in a similar side lying position or in an upright functional position using a resistance band.


Lateral Band Walk - Begin standing with feet shoulder width apart and resistance band around ankles. Knees should be slightly flexed in an athletic stance. Activate core muscles. Take a side step with one leg. Trailing leg should follow to attain shoulder width stance again. Maintain resistance band tension throughout the exercise. Repeat in one direction for 5-10 steps. Return in the opposite direction and repeat 3 times.
Considerations for exercise programming
It is of utmost importance that clients with a history of an ankle sprain be cleared by their physician before starting an exercise program. If the client has completed physical therapy, you can use the exercises that they have learned during their sessions as a good starting point and base for progression or refer to the NASM Essentials of Corrective Exercise book for recommendations.
Here are some general guidelines for working with clients with previous or existing musculoskeletal conditions (21):
- Never exercise through pain.
- Groove appropriate and perfect motion and motor patterns before adding load or other challenges.
- Start by taking gravity out of the equation; start supine or prone, quadruped, kneeling then standing.
- Increase intensity or time, but not both.
- Intensity can be increased by changing either resistance or changing stability.
If the client is ready to be progressed, the following guidelines will help you do this safely and effectively (22):
- If the client is still making progress then continue with the current workload.
- If the client is at plateau then progress at a 2-10% increase.
- If the client experiences a flare-up then decrease volume.
- When working with novice and intermediate clients the recommended volume is 8-12 repetitions for 1-3 sets using 70-85% of 1RM.
As with all exercise programs, long-term adherence and exercise execution on a regular basis are important to achieve satisfying results. After your clients have mastered the movements and are able to maintain good form, you can provide them with short at-home protocols that they can do without equipment to establish regular activity patterns and thus increase their results.
References
- Fong D., et al. 2007. A systematic review on ankle injury and ankle sprain in sports. Sports Med 37(1):73–94.
- Waterman, B., et al. 2010. The Epidemiology of Ankle Sprains in the United States. Bone Joint Surg Am. 92:2279-84
- Drawer, S., Fuller, C. 2001. Propensity for osteoarthritis and lower limb joint pain in retired professional soccer players. Br J Sports Med 35:402-408.
- McKay, G., et al. 2001. Ankle injuries in basketball: injury rate and risk factors. Br J Sports Med 35:103-108.
- Drewes, L., et al. 2008. Dorsiflexion deficit during jogging with Chronic ankle instability. J Sci Med Sport.
- Santos, M., Liu, Wen. 2008. Possible Factors Related to Functional Ankle Instability. JOSPT. 38(3):150-157/
- Friel, K., et al. 2006. Ipsilateral Hip Abductor Weakness After Inversion Ankle Sprain. Journal of Athletic Training. 41(1):74–78.
- Smith, D., et al. 2015 Intra-rater and Inter-rater Reliability and Responsiveness of the Posterior Talar Glide Test. Athletic Training & Sports Health Care 7, 23-28.
- Ekstrand, J., et al. Lower extremity goniometric measurements: A study to determine their reliability. Arch Phys Med Rehab 1982; 63:171-175.
- Garn, S., Newton, R. 1988. Kinesthetic awareness in subjects with multiple ankle sprains. Phys Ther. 68(11):1667-71.
- Byl N. 1992. Spatial orientation to gravity and implication for balance training. Orthopaedic physical therapy clinics of North America. 1(2):207-236
- Bohannon RW, Larkin PA, Cook AC, et al. 1984. Decrease in timed balance test scores with aging. Phys Ther 64:1067- 1075.
- Byl N, Sinnot P. 1991. Variations in balance and body sway in middle-aged adults: subjects with healthy backs compared with subjects with low-back dysfunction. Spine 16:325-30.
- Suni J., Oja P., et al. 1996. Health-related fitness test battery for adults: aspects of reliability. Arch Phys Med Rehabil 77:399-405.
- Agrawal, Y., et al. 2011. The modified Romberg balance test: normative data in US adults. Otol Neurotol. 32(8): 1309–1311.
- Forkin, D., et al. 1996. Evaluation of Kinesthetic Deficits Indicative of Balance Control in Gymnasts with Unilateral Chronic Ankle Sprains. JOSPT 23(4):245-250.
- Clark, M., Lucett, S., Sutton, B. (2014) NASM Essentials of Corrective Exercise Training. Burlington, MA, USA: Jones & Bartlett Learning.
- Vincenzino, B., et al. 2006. Initial Changes in Posterior Talar Glide and Dorsiflexion of the Ankle After Mobilization With Movement in Individuals With Recurrent Ankle Sprain. Orthop Sports Phys Ther. 36(7):464-471.
- Friel, K., et al. 2006. Ipsilateral Hip Abductor Weakness After Inversion Ankle Sprain. Journal of Athletic Training. 41(1):74–78.
- Beckman, S., Buchanan, T. 1995. Ankle inversion injury and hypermobility: Effect on hip and ankle muscle electromyography onset latency. Arch Phys Med Rehab. 76(12):1138-1143.
- Ebig, M., et al. 1997. The Effect of Sudden Inversion Stress on EMG Activity of the Peroneal and Tibialis Anterior Muscles in the Chronically Undstable Ankle. JOSPT. 26(2):73-77.
- Adapted from Blog by Ed LeCara, PhD, DC, MBA, ATC, CSCS.
- American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009 Mar; 41(3):687-708.